
- FY 2023 Enacted levels cited in this document include the effects of the FY 2023 HIV/AIDS transfer, as shown in the Amounts Available for Obligation table.
- Detail in this document may not sum to the subtotals and totals due to rounding.
Director's Overview

The mission of the National Institute of Neurological Disorders and Stroke (NINDS) is to seek fundamental knowledge about the brain and nervous system and to use that knowledge to reduce the burden of neurological disease for all people. The complexity of the brain and nervous system and the substantial collective burden of neurological disorders combine to make this mission a formidable challenge. Our success depends on supporting and conducting rigorous and innovative research that leverages knowledge and tools from multiple scientific disciplines. Just as importantly, ensuring that this research ultimately benefits all people depends on our ability to harness diverse perspectives from an inclusive research workforce and from patients and communities who are directly affected by neurological disorders. Guided by the NINDS 2021-2026 Strategic Plan, urgent public health needs, and promising scientific opportunities, NINDS is investing in neuroscience research for everyone.
Embracing diversity, equity, inclusion, and accessibility
NINDS has long recognized that all of neuroscience benefits if we can engage all segments of society in our efforts. The NINDS Strategic Plan includes goals to ensure a vibrant, talented, and diverse neuroscience workforce and to create and sustain a supportive work culture, and it emphasizes overall that diversity, equity, inclusion, and accessibility (DEIA) are essential to the way we work to fund, conduct, and support research. Consistent with this plan, we are sharpening our focus on actionable steps to enhance DEIA at NINDS and across the research and patient communities we support. Within NINDS, we established an initiative called Culture of Respect and Engagement through Inclusion, Diversity, Equity, Accessibility, and Leadership Support (CORE IDEALS), and as part of the NIH UNITE Initiative, NINDS has developed a dynamic Racial and Ethnic Equity Plan (REEP) that incorporates data-driven strategies and community input to advance racial and ethnic equity at NINDS. We also take a comprehensive approach to enhancing diversity in the extramural neuroscience workforce across the research career pipeline, and a new program seeks to increase diversity among independent investigators funded through Research Project Grants (R01), the mainstay of NIH support for investigator-initiated research. As a model for elevating attention to diversity across other NIH programs, the NIH Brain Research Through Advancing Innovative Neurotechnologies (BRAIN) Initiative® requires most grant proposals to include a Plan for Enhancing Diverse Perspectives (PEDP).1
_______________________________________________
1 Plan for Enhancing Diverse Perspectives (PEDP)
Achieving health equity for neurological disorders
In the United States, the risk of stroke is nearly twice as high for Black people as for White people. Despite overall declines in stroke mortality, Black people have the highest rate of death due to stroke, and Hispanic and American Indian/Alaska Native populations have seen the least improvement over time.2 Hispanic and Black Americans are most at risk for Alzheimer’s disease and related dementias, 3 and the burden of these conditions is expected to increase. The coronavirus disease 2019 (COVID-19) pandemic has accentuated disparities, with less advantaged groups facing greater risks of infection and death, and potentially greater risk for persistent neurological complications. NINDS is committed to understanding and eliminating these and other inequities in the prevalence, health outcomes, and care of neurological disorders, whether associated with different races and ethnicities, religion, socioeconomic status, age, mental health, disability, gender, sexual orientation, gender identity, geographic location, or other characteristics historically linked to discrimination, stigmatization, or exclusion. We are working to address research priorities identified in a new strategic plan for health equity in neurological disorders, with a focus on biologic, sociodemographic, economic, and other determinants of health. For example, two new funding opportunities4 through the NIH Helping to End Addiction Long-term® (HEAL) Initiative aim to support interventions to improve care and outcomes for pain and pain-related comorbidities in populations that experience health disparities. Additional initiatives will support research to test whether lowering vascular risk factors for stroke can also prevent cognitive decline and dementia, especially in racial and ethnic minority groups,5 as well as community-engaged studies to understand how early life social determinants of health (SDOH) and adverse childhood experiences contribute to the development of cognitive impairment and dementia, especially in populations experiencing health disparities.6
_______________________________________________
2 Source: National Vital Statistics Sample 2008-2018 (latest data available as of Oct 2020)
4 RFA-NS-22-002; RFA-NS-22-037
Critical public health challenges and targeted interventions
NINDS is actively engaged in research on some of the greatest public health challenges facing our nation. Among these, NINDS works in close partnership with the National Institute on Aging (NIA) to coordinate and support research on Alzheimer’s disease and Alzheimer’s disease related dementias (AD/ADRD), which include frontotemporal degeneration (FTD), Lewy body dementia (LBD), multiple etiology dementias (MED), and vascular contributions to cognitive impairment and dementia (VCID). In 2022, NINDS led the fourth triennial summit on ADRD to identify updated research priorities, with recommendations for FTD, LBD, MED, and VCID. The summit also addressed opportunities to improve health equity for ADRD and the impact of COVID-19 on AD/ADRD risk and outcomes. Since FY 2016, increased funding for AD/ADRD research has allowed NINDS to expand investigator-initiated research, support opportunities in specific priority areas, and establish collaborative programs and consortia, including efforts focused on the early detection of cognitive impairment and dementia; understanding how stroke, other vascular brain changes, and traumatic brain injury (TBI) affect dementia risk; and identifying FTD and LBD mechanisms and biomarkers. This research is yielding important insights, including recognition that many potential paths to neurodegeneration are shared across conditions, which may inform strategies to prevent or slow disease. Recent studies also suggest that blood-based biomarkers for AD/ADRDs are on the horizon, edging closer to a long-held goal to develop non-invasive measures to aid early intervention.
Launched in 2018, the NIH HEAL Initiative® is an aggressive, trans-agency effort to speed scientific solutions to stem the national opioid public health crisis. As the primary NIH Institute for pain research, NINDS efforts in the HEAL Initiative focus on developing safe, effective non-addictive pain treatments that may mitigate the need for opioids.7 NINDS leads multiple programs within the HEAL Initiative, spanning research supplements to promote research workforce diversity, translational programs for the discovery and development of new treatments, and clinical infrastructure for testing interventions, including the Early Phase Pain Investigation Clinical Network (EPPIC-Net). New therapies are under development and three clinical trials are underway through these NINDS-led programs. In 2022, new awards began through the HEAL Initiative Program to Reveal and Evaluate Cells-to-gene Information that Specify Intricacies, Origins, and the Nature of Human Pain (PRECISION Human Pain). The new network awards support concerted, multidisciplinary team science applying high-throughput analyses to human tissues, with a goal to build comprehensive datasets on molecular and cellular pain signatures that will facilitate the discovery and validation of therapeutic targets.
Given the large and still rising number of Americans affected by COVID-19, research to understand and limit its acute and long-term impacts remains a critical priority. COVID-19-related funding has allowed NINDS intramural and extramural researchers to build knowledge about acute effects of the SARS-CoV-2 virus on the nervous system, as well as persistent, disabling symptoms (Long COVID) lasting weeks or months in some people, such as pain, headaches, fatigue, postural orthostatic tachycardia, sleep disorders, post exertional malaise, and cognitive difficulties. NINDS is also a leading partner in the NIH REsearching COVID to Enhance Recovery (RECOVER) Initiative, established to learn why some people have prolonged symptoms or develop new or returning symptoms after SARS-CoV-2 infection and to inform Long COVID prevention and recovery. Research on Long COVID may shed light on myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), a poorly understood disorder with no effective treatments. Many people with ME/CFS report its onset after an infectious-like illness, and some symptoms associated with Long COVID overlap with those of ME/CFS.
NINDS basic research, on normal nervous system function and disease mechanisms, is the foundation for discovering new cures and preventive interventions. As research homes in on mechanisms behind individual conditions, the potential for targeted therapies grows. For example, existing treatments for epilepsy can have intolerable side effects and are ineffective for about a third of people with epilepsy. Through the Centers Without Walls for Collaborative Research in the Epilepsies, NINDS supports two teams focused on understanding how individual genetic variants cause different types of epilepsy, which will inform new precision therapies. NINDS supports a suite of milestone-driven translational research initiatives to move therapies from target identification to a point of readiness sufficient for industry interest, or in some cases, for testing through NINDS-supported clinical research networks. As recent examples of success, industry investments will advance further development of therapies for pain and epilepsy that were previously supported through the NIH Blueprint Neurotherapeutics Network and the NIH HEAL Initiative Pain Therapeutics Development Program. Among our newest programs, the NINDS Ultra-Rare Gene Therapy (URGenT) Network will bring gene targeting technologies to the development of disease-modifying therapies for ultra-rare disorders, which present unique challenges for therapy development.
_______________________________________________
7 NINDS' Role in the HEAL Initiative
Engaging the community in progress
To drive meaningful advances, the research NINDS supports and conducts must align with priorities of people with lived experience of neurological disorders. Moreover, ensuring that participation in our research is inclusive and accessible is a critical component of our broader DEIA efforts. Consistent with a cross-cutting strategy in the NINDS Strategic Plan, we are strengthening patient and community engagement in NINDS research and have hired dedicated staff to lead in this area. We are working with research and patient communities in priority setting, including as key contributors in new research strategic plans for amyotrophic lateral sclerosis (ALS) and ME/CFS and a recent workshop on cerebral palsy research. In addition, people affected by ALS served on the review committee for a new initiative to support research using data from expanded access to investigational therapies, a provision of the Accelerating Access to Critical Therapies for ALS (ACT for ALS) Act. Also as part of the ACT for ALS, the NIH and the U.S. Food and Drug Administration (FDA) announced a public-private partnership that will convene the ALS community to develop novel strategies for therapy development and clinical testing with the goal to produce a treatment that stops the progression of ALS.8 More broadly, NINDS is developing standard requirements for clinical research studies to include community engagement plans, and NINDS clinical research networks are building community and patient representation into study development and execution. In NIH-wide programs, the HEAL Initiative has adopted innovative approaches to engage people living with pain conditions in clinical research, and the NIH BRAIN Initiative® Neuroethics Working Group held a meeting on addressing the needs of research participants after study protocols end.
_______________________________________________
8 FDA and NIH Launch Public-Private Partnership for Rare Neurodegenerative Diseases
Tackling the undiscovered through powerful science and creative teams
The complexity of the brain and nervous system continues to challenge and inspire researchers. NINDS is a leader in the NIH BRAIN Initiative®, which is applying innovative technologies to learn how brain circuits work. Building on the program’s successes to date, transformative projects are now underway to develop a comprehensive brain cell atlas, a whole mammalian brain microconnectivity map, and tools for precision access to brain cell types. These large-scale projects will open new doors for exploring the brain and, ultimately, for developing new ways to treat and prevent brain diseases. The BRAIN Initiative, the HEAL Initiative, and other NIH programs are demonstrating the power of interdisciplinary teams to solve scientific challenges, and NINDS has established a new program to apply a team-science approach and build new interdisciplinary synergies within our investigator-initiated research portfolio.
Since 2013, the NIH Undiagnosed Diseases Network (UDN) has helped to diagnose nearly 600 perplexing medical conditions, including over 50 newly identified conditions. NINDS has been an important part of the UDN since its inception, given the large number of rare diseases that affect the nervous system. NINDS will now play a leading role in ensuring that this program transitions successfully from the NIH Common Fund to long-term sustainability, including through support for a data management and coordinating center and transitional funding for clinical sites.9 Moving forward, the UDN plans to broaden participation for under/uninsured participants and health disparity populations, integrate the UDN team approach into clinical care, and incorporate additional sites across the country. Advances in genetic research have accelerated discoveries about what causes neurological diseases. However, much remains unknown about non-inheritable factors, including environmental exposure to toxins, social activity and stress, diet, and the microbiome. The new NINDS Office of Neural Exposome and Toxicology (ONETOX) will collaborate across NIH in this growing research area.
_______________________________________________
9 RFA-NS-22-051; RFA-NS-23-004
IC Fact Sheet
View IC Fact Sheet (pdf, 2055 KB)
Major Changes in the Budget Request
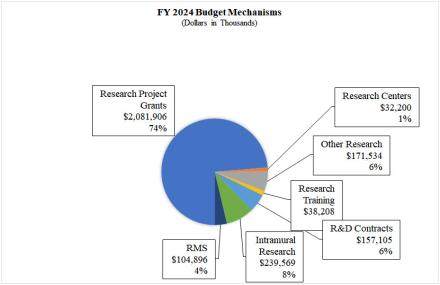
Major changes by budget mechanism and/or budget activity detail are briefly described below. Note that there may be overlap between budget mechanism and activity detail, and these highlights will not sum to the total change for the FY 2024 President’s Budget request for NINDS, which is $2,825.4 million, an increase of $16.0 million from the FY 2023 Enacted level. The request includes $86.0 million provided by the 21st Century Cures Act. Within the President’s Budget request level, NINDS will pursue its highest research priorities through strategic investments and careful stewardship of appropriated funds.
Research Project Grants (RPGs) (+$27.6 million; total $2,081.9 million):
The NINDS budget reflects an increase of $27.6 million in the Research Project Grants portfolio, including SBIR/STTR awards. Competing RPGs are expected to increase by 67 grants in FY 2024 compared to the FY 2023 enacted level of awards.
Research Training (+$2.2 million; total $38.2 million):
NINDS together with the BRAIN Initiative plans to increase the numbers of individual and institutional awards to continue to promote and support the next generation of researchers in neuroscience.
Research and Development Contracts (+$5.2 million; total $157.1 million):
NINDS plans to increase R&D contract funding to accommodate new and expanded contracts within the Biologics and Blueprint Neurotherapeutics Programs.
Intramural Research (-$21.8 million; total $239.6 million):
In FY 2023, a catastrophic flood occurred in the Porter Neuroscience Building, resulting in one-time FY 2023 costs for NINDS to repair damage and restore lost capital equipment and supplies for 18 NINDS laboratories. The FY 2024 request for NINDS intramural research is a reduction from the FY 2023 Enacted level due to phasing out these one-time costs.
Research Management and Support (+$7.2 million; total $104.9 million):
As part of the commitment to effective and efficient stewardship across NINDS programs, the budget reflects an increase of $7.2 million in Research Management and Support to secure additional staff and other support to provide appropriate capacity and oversight for the rapid growth of the NINDS and special initiatives grant portfolio.
Budget Mechanism Table
Budget Mechanism - Total 1,2
(Dollars in Thousands)
| MECHANISM | FY 2022 Final3 | FY 2023 Enacted | FY 2024 President's Budget | FY 2024 +/- FY 2023 | ||||
|---|---|---|---|---|---|---|---|---|
| No. | Amount | No. | Amount | No. | Amount | No. | Amount | |
| Research Projects: | ||||||||
| Noncompeting | 2,227 | $1,171,496 | 2,364 | $1,296,099 | 2,637 | $1,435,897 | 273 | $139,799 |
| Administrative Supplements | (261) | 24,504 | (260) | 23,972 | (265) | 25,496 | (5) | 1,524 |
| Renewal | 110 | 60,183 | 69 | 33,173 | 79 | 53,196 | 10 | 20,023 |
| New | 853 | 559,542 | 735 | 610,901 | 802 | 475,588 | 67 | -135,312 |
| Supplements | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Subtotal, Competing | 963 | $619,725 | 804 | $644,074 | 881 | $528,784 | 77 | -$115,290 |
| Subtotal, RPGs | 3,190 | $1,815,726 | 3,168 | $1,964,144 | 3,518 | $1,990,177 | 350 | $26,033 |
| SBIR/STTR | 115 | 82,901 | 127 | 90,130 | 126 | 91,729 | -1 | 1,599 |
| Research Project Grants | 3,305 | $1,898,626 | 3,295 | $2,054,274 | 3,644 | $2,081,906 | 349 | $27,632 |
| Specialized/Comprehensive | 25 | $31,574 | 26 | $32,082 | 26 | $32,200 | 0 | $118 |
| Clinical Research | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Biotechnology | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Comparative Medicine | 0 | 237 | 0 | 137 | 0 | 0 | 0 | 0 |
| Research Centers in Minority Institutions | 0 | 0 | 0 | 0 | 0 | 0 | 0 | -137 |
| Research Centers | 25 | $31,811 | 26 | $32,220 | 26 | $32,200 | 0 | -$20 |
| Research Careers | 288 | $58,325 | $294 | $58,776 | 300 | $60,669 | 6 | $1,893 |
| Cancer Education | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Cooperative Clinical Research | 0 | 1,948 | 9 | 2,902 | 8 | 1,802 | -1 | -1,101 |
| Biomedical Research Support | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Minority Biomedical Research Support | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Other | 262 | 96,296 | 282 | 114,167 | 291 | 109,064 | 9 | -5,103 |
| Other Research | 550 | $156,570 | 585 | $175,845 | 599 | $171,534 | 14 | -$4,310 |
| Total Research Grants | 3,880 | $2,087,007 | 3,906 | $2,262,339 | 4,269 | $2,285,641 | 363 | $23,302 |
| Individual Awards | 343 | 15,250 | 392 | $17,869 | 397 | $19,494 | 5 | $1,625 |
| Institutional Awards | 285 | 17,517 | 290 | 18,182 | 300 | 18,714 | 10 | 532 |
| Total Research Training | 628 | $32,767 | 682 | $36,051 | 697 | $38,208 | 15 | $2,157 |
Research & Development Contracts | 133 | $157,591 | 134 | $151,891 | 129 | $157,105 | -5 | $5,213 |
| SBIR/STTR (non-add) | (1) | (1,056) | (3) | (1,089) | (3) | (1,099) | (0) | (10) |
| Intramural Research | 321 | 233,988 | 330 | $261,413 | 345 | 239,569 | 15 | -21,844 |
| Research Management and Support | 280 | 95,837 | 302 | 97,724 | 362 | 104,896 | 60 | 7,172 |
| Res. Management & Support (SBIR Admin) (non-add) | (0) | (732) | (0) | (760) | (0) | (789) | (0) | (29) |
| Construction | 0 | 0 | 0 | 0 | ||||
| Buildings and Facilities | 0 | 0 | 0 | 0 | ||||
| Total, NINDS | 601 | $2,607,190 | 632 | $2,809,418 | 707 | $2,825,418 | 75 | $16,000 |
1 All items in italics and brackets are non-add entries.
2 Of which $76.0 million in FY 2022, $225.0 million in FY 2023, and $86.0 million in FY 2024 is derived by transfer from the NIH Innovation Account under the 21st Century Cures Act.
3 Includes $23.4 million of 21st Century Cures Act funding not obligated in FY 2022 and carried over into FY 2023.
Appropriations Language
For carrying out section 301 and title IV of the PHS Act with respect to neurological disorders and stroke, [$2,588,925,000]$2,739,418,00.
NIH INNOVATION ACCOUNT, CURES ACT (INCLUDING TRANSFER OF FUNDS)
For necessary expenses to carry out the purposes described in section 1001(b)(4) of the 21st Century Cures Act, in addition to amounts available for such purposes in the appropriations provided to the NIH in this Act, [$1,085,000,000] $407,000,000, to remain available until expended: Provided, That such amounts are appropriated pursuant to section 1001(b)(3) of such Act, are to be derived from amounts transferred under section 1001(b)(2)(A) of such Act, and may be transferred by the Director of the National Institutes of Health to other accounts of the National Institutes of Health solely for the purposes provided in such Act: Provided further, That upon a determination by the Director that funds transferred pursuant to the previous proviso are not necessary for the purposes provided, such amounts may be transferred back to the Account: Provided further, That the transfer authority provided under this heading is in addition to any other transfer authority provided by law.
Summary of Changes
Summary of Changes
(Dollars in Thousands)
| FY 2023 Enacted | $2,809,418 |
|---|---|
| FY 2024 President's Budget | $2,825,418 |
| Net change | $16,000 |
| FY 2023 Enacted | FY 2024 President's Budget | Built-in Change from FY 2023 CR | ||||
|---|---|---|---|---|---|---|
| CHANGES | FTEs | Budget Authority | FTEs | Budget Authority | FTEs | Budget Authority |
| A. Built-in: 1. Intramural research: | ||||||
| a. Annualization of January 2023 pay increase & benefits | $72,895 | $78,246 | $809 | |||
| b. January FY 2024 pay increase & benefits | 72,895 | 78,246 | 2,794 | |||
| c. Paid days adjustment | 72,895 | 78,246 | 281 | |||
| d. Differences attributable to change in FTE | 72,895 | 78,246 | 3,738 | |||
| e. Payment for centrally furnished services | 34,745 | 35,301 | 556 | |||
| f. Cost of laboratory supplies, materials, other expenses, and non-recurring costs | 153,773 | 126,022 | -18,910 | |||
| Subtotal | -$10,732 | |||||
| 2. RESEARCH MANAGEMENT AND SUPPORT: | ||||||
| a. Annualization of January 2023 pay increase & benefits | $51,904 | $60,705 | $574 | |||
| b. January FY 2024 pay increase & benefits | 51,904 | 60,705 | 1,987 | |||
| c. Paid days adjustment | 51,904 | 60,705 | 200 | |||
| d. Differences attributable to change in FTE | 51,904 | 60,705 | 10,495 | |||
| e. Payment for centrally furnished services | 358 | 364 | 6 | |||
| f. Cost of laboratory supplies, materials, other expenses, and non-recurring costs | 45,462 | 43,827 | 1,023 | |||
| Subtotal | $14,285 | |||||
| Subtotal, Built-in | $3,553 | |||||
| FY 2023 Enacted | FY 2024 President's Budget | Program Change from FY 2023 Enacted | ||||
|---|---|---|---|---|---|---|
| CHANGES | No. | Amount | No. | Amount | No. | Amount |
| B. Program: 1. Research Project Grants: | ||||||
| a. Noncompeting | 2,364 | $1,320,070 | 2,637 | $1,461,393 | 273 | $141,323 |
| b. Competing; | 804 | 644,074 | 881 | 528,784 | 77 | -115,290 |
| c. SBIR/STTR | 127 | 90,130 | 126 | 91,729 | -1 | 1,599 |
| Subtotal, RPGs | 3,295 | $2,054,274 | 3,644 | $2,081,906 | 349 | $27,632 |
| 2. Research Centers | 26 | $32,220 | 26 | 32,200 | 0 | -$20 |
| 3. Other Research | 585 | 175,845 | 599 | 171,534 | 14 | -$4,310 |
| 4. Research Training | 682 | 36,051 | 697 | 38,208 | 15 | 2,157 |
| 5. Research and Development Contracts | 134 | 151,891 | 129 | 157,105 | -5 | 5,213 |
| Subtotal, Extramural | $2,450,281 | $2,480,953 | $30,672 | |||
| 6. Intramural Research | 330 | $261,413 | 345 | $239,569 | 15 | -$11,112 |
| 7. Research Management and Support | 302 | 97,724 | 362 | 104,896 | 60 | -7,113 |
| 8. Construction | 0 | 0 | 0 | |||
| 9. Buildings and Facilities | 0 | 0 | 0 | |||
| Subtotal, Program | 632 | $2,809,418 | 707 | $2,825,418 | 75 | $12,447 |
| Total Changes | $16,000 | |||||
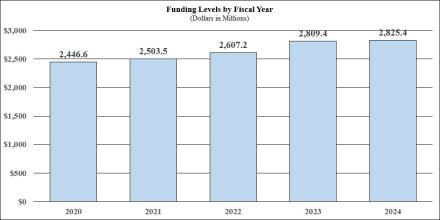
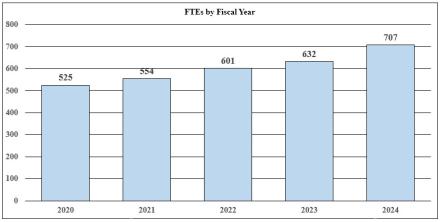
Fiscal Year 2024 Budget Graphs
History of Budget Authority and FTE's:
Distribution of Mechanism:
Change by Selected Mechanism:

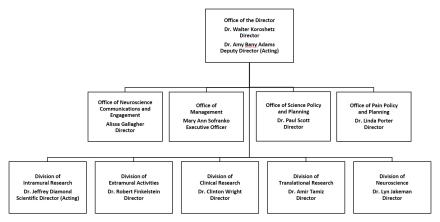
Organization Chart
Budget Authority by Activity
Budget Authority by Activity1
(Dollars in Thousands)
| FY 2022 Final | FY 2023 Enacted | FY 2024 President's Budget | FY 2024 +/- FY 2022 Enacted | |||||
|---|---|---|---|---|---|---|---|---|
| Extramural Research Detail: | FTEs | Amount | FTEs | Amount | FTEs | Amount | FTEs | Amount |
| Division of Neuroscience | $1,612,936 | $1,755,399 | $1,786,427 | $31,027 | ||||
| Division of Clinical Research | 124,982 | 131,100 | 131,193 | 93 | ||||
| Division of Translational Research | 198,602 | 208,322 | 208,469 | 147 | ||||
| Division of Extramural Activities | 103,540 | 108,608 | 108,685 | 77 | ||||
| Opiod Research2 | 237,305 | 246,852 | 246,180 | -$672 | ||||
| Subtotal, Extramural | $2,277,365 | $2,450,281 | $2,480,953 | $30,672 | ||||
Intramural Research | 321 | $233,988 | 330 | $261,413 | 345 | $239,569 | 15 | -$21,844 |
| Research Management & Support | 280 | $95,837 | 302 | $97,724 | 362 | $104,896 | 60 | $7,172 |
| TOTAL | 601 | $2,607,190 | 632 | $2,809,418 | 707 | $2,825,418 | 75 | $16,000 |
1 Includes FTEs whose payroll obligations are supported by the NIH Common Fund.
2 Total for HEAL Initiative including IR and RMS is (in thousands) $270,295 in FY 2022, $280,295 in FY 2023, and $280,295 in FY 2024.
Justification of Budget Request
Justification of Budget Request
National Institute of Neurological Disorders and Stroke
Authorizing Legislation: Section 301 and Title IV of the Public Health Service Act, as amended.
Budget Authority (BA):
| FY 2022 Final | FY 2023 Enacted | FY 2024 President's Budget | FY 2024 +/- FY 2023 | |
|---|---|---|---|---|
| BA | $2,607,190,000 | $2,809,418,000 | $2,825,418,000 | $16,000,000 |
| F T E | 601 | 632 | 707 | 75 |
Program funds are allocated as follows: Competitive Grants/Cooperative Agreements; Contracts; Direct Federal/Intramural and Other.
Overall Budget Policy: The FY 2024 President’s Budget request for NINDS is $2,825.4 million, an increase of $16.0 million or 0.6 percent compared to the FY 2023 Enacted level level. The NINDS request includes 21st Century Cures Act funding of $86.0 million for the BRAIN Initiative. Funding for the HEAL Initiative is equal to the FY 2023 Enacted level of $280.3 million.
Program Descriptions
Extramural Research
Investigator-initiated research driven by scientific opportunity is the foundation for NINDS extramural research, and specific initiatives focus on topics and public health priorities that warrant a more targeted approach. The NINDS Extramural divisions (Division of Neuroscience, Division of Translational Research, Division of Clinical Research, and Division of Extramural Activities) also support research training, resources, core facilities, and scientific conferences.
Division of Neuroscience (DON)
As the largest part of the NINDS extramural program, DON supports research on the normal brain, spinal cord, and nerves of the body; mechanisms of neurological injury and disease; and early development of treatments and diagnostics. DON also supports research resources, core facilities, and scientific conferences. Investigator-initiated research driven by scientific opportunity is the foundation for the DON portfolio, and specific initiatives focus on topics and public health priorities that warrant a more targeted approach. DON program areas include:
- Basic neuroscience research: Gaps in understanding nervous system development and function and disease mechanisms hinder progress in treating and preventing neurological disorders. Basic research to fill those gaps is critical to the NINDS mission and is unlikely to receive sustained support from the private sector. Investing in basic research provides a broad foundation for future breakthroughs. For example, two basic neuroscientists supported by NINDS received the 2021 Nobel Prize in Physiology or Medicine. Over decades of research David Julius and Ardem Patapoutian identified receptors in nerve endings that trigger electrical impulses in response to temperature changes and mechanical force. Beyond unraveling mysteries about how we sense heat, touch, and body position, these fundamental discoveries are leading to new approaches for treating chronic pain and other conditions.
- Neurodegeneration: NINDS leads NIH research support for many neurodegenerative diseases. Programs for Parkinson’s disease include the Morris K. Udall Centers of Excellence; the Parkinson’s Disease Biomarkers Program (PDBP); and the Accelerating Medicines Partnership for Parkinson’s Disease (AMP-PD), which leverages patient cohorts and resources from PDBP and other programs to identify biomarkers and new targets for therapies. As part of the National Plan to Address Alzheimer’s Disease, NINDS leads NIH research on Alzheimer’s Disease Related Dementias (ADRD), which include Lewy Body dementia (LBD), frontotemporal dementia, vascular contributions to cognitive impairment and dementia (VCID), and mixed etiology dementias. Co-funding from the National Institute on Aging (NIA) enables support for specific initiatives and an extended payline for meritorious ADRD research proposals. NINDS is also partnering with the NIH Common Fund on the Accelerating Leading-edge Science in ALS (ALS2) initiative, which supported four new projects in 2021 on new mechanistic insights, finding target genes for therapeutic intervention, assessing a way to slow progression, and how environmental exposures contribute to ALS risk.
- Stroke and cerebrovascular disease:NINDS supports a broad portfolio of research to understand stroke causes and the mechanisms involved in stroke-related damage and repair, which might be harnessed to aid neuroprotection and recovery. NINDS established the Stroke Preclinical Assessment Network (SPAN) to rigorously test potential neuroprotective therapies in rodent models of acute ischemic stroke, with built-in replication studies across multiple laboratories to ensure unbiased results. Therapies that are successful in SPAN may later move into clinical trials through the NIH StrokeNet, a NINDS-funded network for stroke clinical trials. NINDS stroke research includes studies to understand small vessel disease (SVD) in the brain, which affects the brain’s small arteries and veins. In addition to stroke, SVD is a major cause of VCID. Together with NIA, NINDS also supports a national consortium called MarkVCID to develop and evaluate biomarkers that will help predict, diagnose, and track VCID.
- Rare diseases: Many rare diseases affect the nervous system, and research on these disorders often yields insights into more common diseases with shared mechanisms. NINDS supports a large portfolio of research on rare diseases and is a partner in the NIH Rare Diseases Clinical Research Network, funding consortia for lysosomal disorders, mitochondrial diseases, dystonia, and others. NINDS has contributed to new treatments for rare disorders, including the first gene-based, disease-modifying therapies for spinal muscular atrophy and muscular dystrophy. An ongoing NINDS initiative aims to fill gaps in clinical trial readiness for rare neurological and neuro-muscular diseases with new therapies on the horizon, and a new initiative will support natural history and clinical outcome assessment studies for ultra-rare neurological diseases, meeting a critical need for therapy development. In FY 2023, NINDS will lead NIH support for a data management and coordinating center for the Undiagnosed Disease Network, enabling this successful program to continue past its initial NIH Common Fund support.
- Other neurological disorders: DON research includes studies on many more nervous system disorders and on mechanisms shared across diseases, with studies informing new and improved treatments and diagnostics for hydrocephalus, spinal cord injury, traumatic brain injury (TBI), and neuropathies, among others. NINDS seeks input from research and patient communities to help set priorities, such as the Benchmarks for Epilepsy Research, updated in 2020. Because neuroscience spans scientific disciplines, NINDS also works closely with other NIH Institutes in areas of complementary interest. For example, in addition to having a leading role in the NIH HEAL InitiativeSM, NINDS is the primary NIH Institute for pain and headache research and leads the NIH Pain Consortium, which includes 23 Institutes and Centers. NINDS also leads NIH efforts focused on myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), including support for multi-disciplinary research centers focused on understanding this complex disease and building research capacity. Additional areas of collaboration include developmental disorders such as cerebral palsy, autism, Fragile X Syndrome, and Down syndrome; muscular dystrophies; brain tumor; autoimmune conditions such as multiple sclerosis (MS); and infections that affect the nervous system, including acute and long-term effects of COVID-19.
The Brain Research Through Advancing Innovative Neurotechnologies® (BRAIN) Initiative The NIH BRAIN Initiative® is an ambitious program to develop and apply new tools and technologies to fundamental questions about the brain and ultimately to inspire new treatments for brain diseases. NINDS and NIMH are lead partners in the NIH BRAIN Initiative, working with eight other Institutes and Centers. With Congressional support, including funding authorized by the 21st Century Cures Act, the BRAIN Initiative has invested over $3 billion in more than 1,300 research projects, engaging scientists from many areas of expertise as well as mathematicians, engineers, physicians in individual labs and interdisciplinary teams. The BRAIN Initiative has also led positive change in the culture of neuroscience research through its emphasis on neuroethics, diversity and inclusion, and promoting infrastructure and practices for sharing research data and tools.
Tools and technologies developed through the BRAIN Initiative are helping researchers understand complex cognitive functions, investigate disease mechanisms, and develop and improve clinical applications.
- Over 250 scientists at more than 45 institutions across three continents collaborated in the BRAIN Initiative® Cell Census Network (BICCN), which created an atlas of cell types and a neuronal wiring diagram for the mammalian primary motor cortex.
- Tools developed by the BICCN are aiding new discoveries on cell types that degenerate in Alzheimer’s and Parkinson’s disease, providing clues for future interventions that may one day slow or even halt disease progression.
- New approaches for recording brain activity show how the brain stores and recalls distinct events and how brain circuitry can layer memories of events over more stable memories of spatial environments.
- BRAIN research is fueling advances in adaptive, individualized brain stimulation for movement disorders, epilepsy, chronic pain, obsessive compulsive disorder, and depression, as well as brain-computer devices to aid communication in people who cannot speak.
Three large-scale transformative projects will build on progress: The BRAIN Initiative Cell Atlas Network (BICAN), to generate an atlas of human brain cell types across the lifespan; the Armamentarium for Precision Brain Cell Access, to build a toolkit for researchers to access specific cells and circuits in model systems and human tissue specimens; and the BRAIN Initiative Connectivity Across Scales (BRAIN CONNECTS) Network, to grow research and technical capacity to generate wiring diagrams that span entire brains. In addition, BRAIN continues to support projects that shift technology from the bench to clinical settings and projects in new focus areas, including a more complete understanding of the neural circuit basis of behavior.
Budget Policy: The FY 2024 President’s Budget request for the Division of Neuroscience is $1,786.4 million, an increase of $31.0 million, or 1.8 percent, from the FY 2023 Enacted level.
Division of Translational Research (DTR)
The DTR leads extramural NINDS therapy development through milestone-driven programs and services that support all development stages for drugs, devices, and biologic therapies, from preclinical studies to first-in-human clinical trials. Translational research is prone to failure and poses risks for private sector investment. DTR programs help to remove these risks by advancing therapies to a point of readiness sufficient for industry interest, or in some cases, for testing in NINDS-funded clinical trials. DTR will support the following programs in FY 2024: .
- The Blueprint Neurotherapeutics Network (BPN), led by NINDS for the NIH Blueprint for Neuroscience Research, supports small molecule drug development. Recent industry investment in BPN-funded strategies for epilepsy and pain show that this program is helping to bring therapies closer to the clinic. New BPN projects focus on promoting nerve growth after spinal cord injury and preventing post-seizure cognitive deficits.
- The Innovation Grants to Nurture Initial Translational Efforts (IGNITE) program funds early-stage therapy development that fuels the pipeline for later stage programs, such as BPN. IGNITE activities include assay validation, demonstrating biological activity sufficient to merit further study, and model system development for early testing.
- The Blueprint Neurotherapeutics Network for Biologics (BPN-Biologics) advances biological therapies, including large biological molecules, cell therapies, and gene-targeted therapies. New projects aim to develop treatments for spinal muscular atrophy and for producing on-demand voiding in people with bowel or bladder retention due to spinal cord injury or other diseases. The NINDS Translational Neural Devices program supports therapeutic and diagnostic device development for nervous system disorders, from preclinical studies through early-stage clinical trials. In 2021, NINDS and the NIH Blueprint for Neuroscience Research announced the Blueprint MedTech program as an incubator for cutting-edge neurotechnology.
- The NINDS Ultra-rare Gene Therapy (URGenT) Network supports precision medicine therapy development for serious, life-threatening ultra-rare neurological diseases affecting fewer than 20 in one million people. Together, these diseases represent a large medical need without available treatments and with little incentive for private sector therapy development.
- The NINDS Biomarkers supports development and validation of biomarkers for use in clinical trials to aid therapy development or to help guide patient care decisions. Projects in advanced validation stages include biomarkers for MS diagnosis and monitoring, TBI prognosis, and differential diagnosis of three different forms of Parkinsonism.
- The Epilepsy Therapy Screening Program (ETSP) tests compounds from academic institutions and industry in well characterized models of epilepsy and has contributed to 11 marketed drugs for the treatment of epileptic seizures. The ETSP aims to advance novel therapies to prevent epilepsy, modify disease progression, and treat drug-resistant epilepsy.
- Small Business Innovation Research (SBIR) and Small Business Technology Transfer (STTR) Programs support research by small businesses on therapies, diagnostics, and research tools relevant to the NINDS mission. Many DTR programs, as well as the NIH BRAIN® and HEAL® initiatives, include SBIR/STTR components. Among recent successes is a new FDA-cleared product called Nerve Tape® for sutureless repair of injured nerves.
- The new Office of Neural Exposome and Toxicology (ONETOX) will focus on the role of non-inheritable factors in neurological diseases, including environmental exposure to toxins, social activity and stress, diet, and the microbiome. ONETOX also oversees the NIH Countermeasures Against Chemical Threats (CounterACT) program, funded by the NIH Office of the Director and part of the Chemical Countermeasures Research Program at the National Institute of Allergy and Infectious Diseases (NIAID)..
Budget Policy: The FY 2024 President’s Budget request for the Division of Translational Research is $208.5 million, an increase of $0.1 million, or 0.1 percent, from the FY 2023 Enacted level.
Division of Clinical Research (DCR)
DCR supports clinical trials infrastructure and large-scale clinical research, including early and advanced phase clinical trials, comparative effectiveness research, and epidemiological studies for neurological conditions across the lifespan. NINDS clinical research networks provide infrastructure for efficient early and late stage multi-site clinical trials, bring together expert communities to promote high-quality research, enable partnerships with industry and patient groups, and help train future clinical trial investigators. In FY 2024, DCR programs will include:
NINDS clinical research networks provide accessible infrastructure for efficient early and late stage clinical trials, bring together expert communities to promote high-quality research, enable partnerships with industry and patient groups, and help train future clinical trial investigators.
- The Network for Excellence in Neuroscience Clinical Trials (NeuroNext) supports Phase II clinical trials to test investigational treatments prior to larger late-stage trials, as well as studies to discover and validate biomarkers. Since 2011, NeuroNEXT has initiated 11 studies focused on a range of common and rare neurological disorders. Completed trials have built evidence to justify later stage trials for treatments for MS, Huntington’s disease, neuroprotection after acute stroke, and GNE myopathy, a rare muscle disease. A prior biomarker and natural history study on spinal muscular atrophy contributed to the approval of the first treatment for this disease.
- NIH StrokeNet supports trials on stroke treatment, prevention, and recovery and rehabilitation through 26 regional centers and over 500 hospitals. Since 2014, the network has conducted 20 trials and contributed to two trials through the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) public-private partnership. Trial results are informing clinical care, including a landmark study showing that surgical removal (endovascular thrombectomy, or EVT) of large vessel blockages can be effective in brain-imaging selected patients up to 16 hours after stroke onset. To assess the potential benefits of expanding this intervention to more patients and to explore innovative methods to augment outcomes and improve systems of care, StrokeNet added a novel EVT Platform in 2022 that will use StrokeNet infrastructure to efficiently and simultaneously test several interventions.
- Strategies to Innovate EmeRgENcy Care Clinical Trials Network (SIREN), led by NINDS and the National Heart, Lung, and Blood Institute (NHLBI), conducts clinical trials in emergency care for neurologic, cardiac, respiratory, and hematologic conditions. Ongoing trials are testing treatments for traumatic brain Injury (TBI) and improving neurological outcomes after cardiac arrest in adults, and a new study is addressing cardiac arrest in children. Other new projects are studying EEG patterns and biomarkers for clinical monitoring in patients in a coma after TBI.
- The Office of Global Health and Health Disparities within DCR directs NINDS support for research on health disparities for neurological disorders and on minority, community, and global health relevant to the NINDS mission. A new strategic plan for research on health disparities and health equity for neurological disorders will guide and strengthen new NINDS investments.
- The Prospective Observational Comparative Effectiveness Reearch in Clinical Neurosciences initiative launched its first study in 2022. Comparing Treatment Approaches to Promote Inpatient Rehabilitation Effectiveness for Traumatic Brain Injury (CARE 4 TBI) will compare specific inpatient rehabilitation approaches for people with TBI to optimize functional outcomes and community participation.
- The NINDS Common Data Elements (CDE) Program works with researchers, industry, other Federal agencies, and nonprofit and professional organizations to develop data standards for neurological disorders, to foster collaboration and data sharing across studies, and improve data quality and integrity. The program has developed CDEs for more than 20 disease areas, many with pediatric standards, and a common set for use across diseases. New or updated CDEs are underway for TBI, coma, social determinants of health, and mitochondrial disorders.
Budget Policy: The FY 2024 President’s Budget request for the Division of Clinical Research is $131.2 million, an increase of $0.1 million, or 0.1 percent, from the FY 2023 Enacted level.
Division of Extramural Activities (DEA)
DEA leads extramural NINDS efforts in research training and career development, workforce development, and enhancing research rigor, that together fuel capacity for innovative neuroscience research for generations to come. DEA also houses the NINDS Scientific Review Branch and the Office of Research Operations and Analysis, including grants management and analytical and administrative functions for effective implementation of NINDS programs and policies.
- The Office of Programs to Enhance Neuroscience Workforce (OPEN) represents NINDS at all levels of NIH in matters pertaining to training and workforce development in the extramural biomedical workforce. OPEN develops and implements individual and institutional funding opportunities while working across the NINDS, Blueprint, and BRAIN scientific portfolios to promote the scientific workforce in the neurosciences. OPEN develops training opportunities and organizes conferences, workshops, symposia, and professional development activities to enhance participation in the neuroscience workforce.
- The Office of Training and Workforce Development directs NINDS extramural research training and career development, including fellowships, mentored awards, and programs at academic institutions. NINDS initiatives complement NIH-wide programs to address unique training needs across neuroscience research career stages and include national research training programs for neurosurgeons and pediatric neurologists, career development awards for advanced trainees launching independent projects, and workshops focused on strengthening mentorship in neuroscience research. In collaboration with OPEN, the NIH Neuroscience Doctoral Readiness Program (DR. Program)11 will support postbaccalaureate research experiences for a diverse cadre of students who have not had access to substantive research opportunities, with a goal to enable successful transition into strong, research-focused doctoral degree programs in biomedical fields.
- The Office of Research Quality promotes rigor and transparency in neuroscience research and has been instrumental to NIH and research journal policies to improve rigor in experimental design and transparent reporting in publications. New initiatives12 support community-driven development of innovative educational materials that will be incorporated into an openly accessible online resource to promote awareness, understanding, and practice of fundamental principles of rigorous research for scientists in various career stages and learning environments.
Budget Policy: The FY 2024 President’s Budget request for the Division of Extramural Activities is $108.7 million, an increase of $0.1 million, or 0.1 percent, from the FY 2023 Enacted level.
_______________________________________________
10 NINDS Diversity Awards
12 RFA-NS-21-033; RFA-NS-21-009
NIH Helping to End Addiction Long-termSM (HEAL) Initiative
The NIH HEAL Initiative is a trans-agency effort to speed scientific solutions to stem the national opioid crisis. As the NIH lead for pain research, NINDS HEAL Initiative activities focus on developing non-addictive and effective pain treatments that may mitigate the need for opioids for pain management. NINDS also supports HEAL programs for research training and career development to promote a diverse, dedicated workforce to address evolving opioid and pain public health challenges. NINDS HEAL efforts13 include other NIH ICOs as partners, and they build on and integrate with NINDS programs for basic, translational, and clinical research.
A suite of milestone-driven programs, including the Pain Therapeutic Development Program (PTDP), support the discovery, optimization, and development of non-addictive small molecule and biologic therapies to treat pain. In addition, the Preclinical Screening Platform for Pain (PSPP) tests and characterizes promising non-addictive therapeutic candidates submitted by researchers (small molecules, biologics, or natural products) in animal models that mimic a variety of human pain conditions. Parallel programs support the development of device-based approaches for treating pain and improving pain management. NINDS also leads a HEAL Initiative® program to support the development of biomarkers that can predict or monitor response to pain therapeutics, which will facilitate clinical trials to test new therapies.
The Early Phase Pain Investigation Network (EPPIC-Net) provides infrastructure for the rapid design and performance of Phase II clinical trials to test novel and promising therapeutics for pain, as well as phenotyping and biomarker studies in people with specific pain conditions. EPPIC-Net has launched one clinical trial for knee osteoarthritis pain and will launch two trials for diabetic peripheral neuropathy. NINDS also plays a lead role in the Pain Management Effectiveness Research Network, which supports clinical trials on the comparative effectiveness of existing pharmacological and non-pharmacological therapies for pain management while mitigating the use of opioids. Furthermore, NINDS is a key partner in HEAL efforts to reduce health equities in pain care, with studies to develop, test, and implement interventions to improve outcomes and access to quality pain care in populations that experience health disparities.
Budget Policy: The FY 2024 President’s Budget request for NINDS HEAL is $280.3 million, equal to the FY 2023 Enacted level. NINDS HEAL funding for FY 2024 includes $246.2 million for extramural research, $20.0 million for intramural research, and $14.1 million for RMS.
_______________________________________________
13 NINDS Diversity Awards
Intramural Research Program (IRP)
The NINDS IRP conducts research and research training on the NIH campus, spanning basic, translational, and clinical research in neuroscience, neurology, and neurosurgery and hosting state-of-the-art core facilities. The IRP’s unique resources enable innovative, multidisciplinary studies to answer fundamental questions about the nervous system and its diseases; and with over 150 neuroscience research labs from NINDS and 10 other Institutes, including many co-located in the Porter Neuroscience Research Center, the IRP is a rich environment for collaboration.
NINDS investigators recently described novel imaging approaches for monitoring microbleeds due to viral infections in the brain. This research advances our understanding of infections and immune responses in the brain and may aid the development of immune-based therapies for brain infections and cancers.14 In another study, researchers reported a new type of interaction between cholinergic and dopaminergic signaling, two neurotransmitter systems in the brain. The findings have implications for understanding normal cognitive functions such as reward, motivation, and motor learning, as well as in disorders such as Parkinson’s disease.15
NINDS intramural clinical studies benefit from the NIH Clinical Center, a hospital devoted solely to clinical research, and from collaboration with local hospitals and extramural scientists. NINDS leads a multisystem study on post-infectious ME/CFS to identify clinical and biological markers and disease mechanisms, a study of veterans with Gulf War Illness (with the Veterans Health Administration), and a study of people with persistent symptoms after acute COVID-19 infection. Other clinical studies focus on stroke and VCID, neurodegenerative diseases, MS, TBI, epilepsy, brain tumors, movement disorders, and rare genetic disorders, and include early trials for drugs, devices, and gene therapy. In addition, NINDS helps find causes of puzzling neurological cases through the NIH Undiagnosed Diseases Program.
The Roy Blunt Center for Alzheimer’s and Related Dementias (CARD),16 established by NIA and NINDS in 2020, will stimulate ambitious research that may be challenging within traditional extramural mechanisms. Understanding the many ways genes linked to neurodegeneration affect cellular pathways will be essential for finding strategies to prevent or halt disease. CARD is using cutting-edge genetic methods to create a freely available research repository of induced pluripotent stem cell lines modeling over 100 different AD/ADRD gene variants. Among other projects, CARD scientists are also developing a therapeutic strategy designed to clear cellular aggregates of the protein Tau, a pathological hallmark of Alzheimer’s and related dementias.
Budget Policy: The FY 2024 President’s Budget request for the Intramural Research Program is $239.6 million, a decrease of $21.8 million, or 8.4 percent, from the FY 2023 Enacted level.
_______________________________________________
14 Early detection of cerebrovascular pathology and protective antiviral immunity by MRI
16 NIH Intramural Center for Alzheimer’s and Related Dementias (CARD)
Research Management and Support (RMS)
RMS comprises administrative, budgetary, logistical, and scientific support in the review, award, and monitoring of research grants, training awards, and research contracts. RMS also includes strategic planning, program evaluation, regulatory compliance, enhanced patient and community engagement activities, internal DEIA efforts, communication about neurological disorders and NINDS research, and liaison with other agencies, Congress, and the public. In 2021, NINDS updated its stroke prevention campaign (Mind Your Risks), based on evidence linking high blood pressure (hypertension) and the risk of dementia later in life. Updated messaging aims to engage young Black men, to help address high risks for stroke and dementia in Black Americans.
Budget Policy: The FY 2024 President’s Budget request for Research Management and Support is $104.9 million, an increase of $7.2 million, or 7.3 percent, from the FY 2023 Enacted level.
Appropriations History
| Fiscal Year | Budget Estimate to Congress | House Allowance | Senate Allowance | Appropriation |
|---|---|---|---|---|
| 2015 | $1,608,461,000 | $1,605,205,000 | ||
| Rescission | $0 | |||
| 2016 | $1,660,375,000 | $1,656,334,000 | $1,694,758,000 | $1,696,139,000 |
| Rescission | $0 | |||
| 20171 | $1,695,180,000 | $1,751,049,000 | $1,803,306,000 | $1,783,654,000 |
| Rescission | $0 | |||
| 20182 | $1,355,998,000 | $1,853,011,000 | $1,904,666,000 | $2,188,149,000 |
| Rescission | $0 | |||
| 20192 | $1,838,556,000 | $2,228,780,000 | $2,275,580,000 | $2,274,413,000 |
| Rescission | $0 | |||
| 20202 | $2,026,031,000 | $2,385,571,000 | $2,490,494,000 | $2,444,687,000 |
| Recission | $0 | |||
| 20212 | $2,245,110,000 | $2,465,110,00 | $2,526,245,000 | $2,513,393,000 |
| Recission | $0 | |||
| 20222 | $2,783,300,000 | $2,799,515,000 | $2,786,096,000 | $2,611,370,000 |
| Recission | $0 | |||
| 20232 | $2,768,043,000 | $2,833,590,000 | $2,765,918,000 | $2,813,925,000 |
| Recission | $0 | |||
| 20232 | $2,825,418,000 |
1 Budget Estimates to Congress includes mandatory financing.
2 Includes funds derived by transfer from the NIH Innovation Account under the 21st Century Cures Act.
Authorizing Legislation
| PHS Act/ Other Citation | U.S. Code Citation | 2023 Amount Authorized | FY 2023 Enacted | 2024 Amount Authorized | F Y 2024 President's Budget | |
|---|---|---|---|---|---|---|
| Research and Investigation | Section 301 | 42§241 | Indefinite | $2,809,418,000 | Indefinite | $2,825,418,000 |
| National Institute of Neurological Disorders and Stroke | Section 401(a) | 42§281 | Indefinite | Indefinite | ||
| Total, Budget Authority | $2,809,418,000 | $2,825,418,000 |
Amounts Available for Obligation
Amounts Available for Obligation 1
(Dollars in Thousands)
| Source of Funding | FY 2022 Final | FY 2023 Enacted | FY 2024 President's Budget |
|---|---|---|---|
| Appropriation2 | $2,611,370 | $2,813,925 | $2,825,418 |
| OAR HIV/AIDS Transfers | -$4,180 | -$4,507 | $0 |
| Subtotal, adjusted budget authority | $2,607,190 | $2,809,418 | $2,825,418 |
| Unobligated balance, start of year | $21,103 | $33,120 | $0 |
| Unobligated balance, end of year (carryover)3 | -$33,120 | $0 | $0 |
| Subtotal, adjusted budget authority | $2,595,173 | 2,842,538 | 2,825,418 |
| Unobligated balance lapsing | -$10 | $0 | $0 |
| Total obligations | $2,595,163 | $2,842,538 | $2,825,418 |
1 Excludes the following amounts (in thousands) for reimbursable activities carried out by this account:
FY 2022 - $27,981 FY 2023 - $30,978 FY 2024 - $32,000
2 Of which $76.0 million in FY 2022, $225.0 million in FY 2023, and $86.0 million in FY 2024 is derived by transfer from the NIH Innovation Account under the 21st Century Cures Act.
3 Reflects 21st Century Cures Act funding not obligated in FY 2022, and carried over into FY 2023.
Budget Authority by Object Class
Budget Authority by Object Class 1
(Dollars in Thousands)
| FY 2023 Enacted | FY 2024 President's Budget | FY 2024 +/- FY 2023 | |
|---|---|---|---|
| Total compensable workyears: | |||
| Full-time equivalent | 632 | 707 | 75 |
| Full-time equivalent of overtime and holiday hours | 0 | 0 | 0 |
| Average ES salary | $184 | $184 | $1 |
| Average GM/GS grade | 12.9 | 12.9 | 0.0 |
| Average GM/GS salary | $130 | $138 | $7 |
| Average salary, Commissioned Corps (42 U.S.C. 207) | $0 | $0 | $0 |
| Average salary of ungraded positions (in whole dollars) | $146 | $148 | $2 |
OBJECT CLASSES | FY 2023 Enacted | FY 2024 President's Budget | FY 2024+/- FY 2023 |
|---|---|---|---|
| Personnel Compensation: | |||
| 11.1 Full-time permanent | $47,202 | $53,970 | $6,768 |
| 11.3 Other than full-time permanent | 30,746 | 33,473 | 2,726 |
| 11.5 Other personnel compensation | 3,598 | 4,001 | 403 |
| 11.7 Military personnel | 164 | 177 | 13 |
| 11.8 Special Personnel Services Payments | 12,214 | 12,880 | 666 |
| 11.9 Subtotal Personnel Compensation | $95,181 | $104,501 | $10,577 |
| 12.1 Civilian Personnel benefits | 30,820 | 34,392 | 3,572 |
| 12.2 Military Personnel Benefits | 54 | 58 | 4 |
| 13.0 Benefits to Former Personnel | 0 | 0 | 0 |
| Subtotal, Pay Costs | $124,798 | $138,951 | $14,153 |
| 21.0 Travel and Transportation of Persons | 2,247 | 2,301 | 54 |
| 22.0 Transportation of Things | 379 | 388 | 9 |
| 23.1 Rental Payments to GSA | 0 | 0 | 0 |
| 23.2 Rental Payments to Others | 56 | 57 | 1 |
| 23.3 Communications, Utilities and Miscellaneous Charges | 257 | 263 | 6 |
| 24.0 Printing & Reproduction | 0 | 0 | 0 |
| 25.1 Consulting Services | 52,670 | 53,569 | 899 |
| 25.2 Other Services | 56,311 | 53,462 | -2,849 |
| 25.3 Purchase of goods and services from government accounts | 191,996 | 193,141 | 1,146 |
| 25.4 Operation & Maintenance of Facilities | 697 | 707 | 10 |
| 25.5 R&D Contracts | 40,625 | 34,051 | 6,574 |
| 25.6 Medical Care | 290 | 302 | 12 |
| 25.7 Operation & Maintenance of Equipment | 4,420 | 4,084 | -337 |
| 25.8 Subsistence & Support of Persons | 0 | 0 | 0 |
| 25.0 Subtotal Other Contractual Services | $347,008 | $339,316 | -$7,693 |
| 26.0 Supplies & Materials | $17,490 | $12,672 | $4,818 |
| 31.0 Equipment | 26,859 | 6,034 | -20,825 |
| 32.0 Land and Structures | 1,538 | 1,575 | 37 |
| 33.0 Investments & Loans | 0 | 0 | 0 |
| 41.0 Grants, Subsidies & Contributions | 2,288,773 | 2,323,849 | 35,076 |
| 42.0 Insurance Claims & Indemnities | 0 | 0 | 0 |
| 43.0 Interest & Dividends | 12 | 12 | 0 |
| 44.0 Refunds | 0 | 0 | 0 |
| Subtotal Non-Pay Costs | $2,684,620 | $2,686,467 | $1,847 |
| Total Budget Authority by Object Class | $2,809,418 | $2,825,418 | $16,000 |
1Includes FTEs whose payroll obligations are supported by the NIH Common Fund.
Salaries and Expenses
Salaries and Expenses
(Dollars in Thousands)
| OBJECT CLASSES | FY 2023 Enacted | FY 2024 President's Budget | FY 2024 +/- FY 2023 |
|---|---|---|---|
| Personnel Compensation: | |||
| Other Contractual Services: | |||
| Full-Time Permanent (11.1) | $47,202 | $53,970 | $6,768 |
| Other Than Full-Time Permanent (11.3) | 30,746 | 33,473 | 2,726 |
| Other Personnel Compensation (11.5) | 3,598 | 4,001 | 403 |
| Military Personnel (11.7) | 164 | 177 | 13 |
| Special Personnel Services Payments (11.8) | 12,214 | 12,880 | 666 |
| Subtotal Personnel Compensation (11.9) | $93,924 | $104,501 | $10,577 |
| Civilian Personnel Benefits (12.1) | $30,820 | $34,392 | $3,572 |
| Military Personnel Benefits (12.2) | 54 | 58 | 4 |
| Benefits to Former Personnel (13.0) | 0 | 0 | 0 |
| Subtotal Pay Costs | $124,798 | $138,951 | $14,153 |
| Travel & Transportation of Persons (21.0) | $2,247 | $2,301 | $54 |
| Transportation of Things (22.0) | 379 | 388 | 9 |
| Rental Payments to Others (23.2) | 56 | 57 | 1 |
| Communications, Utilities and Misc. Charges (23.3) | 257 | 263 | 6 |
| Printing and Reproduction (24.0) | 0 | 0 | 0 |
| Consultant Services (25.1) | 52,400 | 53,292 | 893 |
| Other Services (25.2) | 56,311 | 53,462 | 2,849 |
| Purchases from government accounts (25.3) | 103,473 | 102,880 | -593 |
| Operation and Maintenance of Facilities (25.4) | 697 | 707 | 10 |
| Operation and Maintenance of Equipment (25.7) | 4,420 | 4,084 | -337 |
| Subsistence and Support of Persons (25.8) | 0 | 0 | 0 |
| Subtotal Other Contractual Services | $217,301 | $214,425 | -$2,876 |
| Supplies and Materials (26.0) | $17,490 | $12,672 | -$4,818 |
| Subtotal Non-Pay Costs | $237,729 | $230,106 | -$7,623 |
| Total Administrative Costs | $362,527 | $369,057 | $6,530 |
Detail of Full-Time Equivalent Employment (FTE's)
Detail of Full-Time Equivalent Employment (FTE's)
| OFFICE/DIVISION | FY 2022 Final | FY 2023 Enacted | FY 2024 President's Budget | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Civilian | Military | Total | Civilian | Military | Total | Civilian | Military | Total | |
| Office of the Director | |||||||||
| Division of Clinical Research | |||||||||
| Division of Translational Research | |||||||||
| Division of Intramural Research | |||||||||
| Division of Extramural Activities | |||||||||
| Division of Neuroscience | |||||||||
| Includes FTEs whose payroll obligations are supported by the NIH Common Fund. | |||||||||
| Direct: | 76 | - | 76 | 70 | - | 70 | 85 | - | 85 |
| Reimbursable: | 7 | - | 7 | 14 | - | 14 | 16 | - | 16 |
| Total: | 83 | - | 83 | 84 | 84 | 101 | - | 101 | |
| Direct: | 24 | - | 24 | 27 | - | 27 | 32 | - | 32 |
| Reimbursable: | - | - | - | 1 | - | 1 | 2 | - | 2 |
| Total: | 24 | - | 24 | 28 | - | 28 | 34 | - | 34 |
| Direct: | 32 | - | 32 | 45 | - | 45 | 56 | - | 56 |
| Reimbursable: | 4 | - | 4 | 4 | - | 4 | 4 | - | 4 |
| Total: | 36 | - | 36 | 49 | - | 49 | 60 | - | 60 |
| Direct: | 304 | 1 | 305 | 312 | - | 312 | 328 | - | 328 |
| Reimbursable: | 16 | - | 16 | 18 | - | 18 | 17 | - | 17 |
| Total: | 320 | 1 | 321 | 330 | - | 330 | 345 | - | 345 |
| Direct: | 80 | - | 80 | 80 | - | 80 | 95 | - | 95 |
| Reimbursable: | - | - | - | - | - | - | 1 | - | 1 |
| Total: | 80 | - | 80 | 80 | - | 80 | 96 | - | 96 |
| Direct: | 50 | - | 50 | 50 | - | 50 | 59 | - | 59 |
| Reimbursable: | 7 | - | 7 | 11 | - | 11 | 12 | - | 12 |
| Total: | 57 | - | 57 | 61 | - | 61 | 71 | - | 71 |
| Total | 600 | 1 | 601 | 632 | - | 632 | 707 | - | 707 |
| FTEs supported by funds from Cooperative Research and Development Agreements | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
FTEs supported by funds from Cooperative Research and Development Agreements.
| FISCAL YEAR | Average GS Grade |
|---|---|
| 2020 | 12.6 |
| 2021 | 13.8 |
| 2022 | 12.8 |
| 2023 | 12.9 |
| 2024 | 12.9 |
Detail of Positions
Detail of Positions1
(Dollars in Thousands)
| GRADE | FY 2022 Final | FY 2023 Enacted | FY 2024 President's Budget |
|---|---|---|---|
| Total, ES Positions | 1 | 1 | 1 |
| Total, ES Salary | 182,850 | 183,500 | 184,152 |
| GM/GS-15 | 66 | 66 | 66 |
| GM/GS-14 | 99 | 107 | 116 |
| GM/GS-13 | 134 | 144 | 157 |
| GS-12 | 70 | 75 | 82 |
| GS-11 | 34 | 34 | 34 |
| GS-10 | 1 | 1 | 1 |
| GS-9 | 13 | 13 | 13 |
| GS-8 | 3 | 3 | 3 |
| GS-7 | 5 | 5 | 5 |
| GS-6 | 1 | 1 | 1 |
| GS-5 | 1 | 1 | 1 |
| GS-4 | 2 | 2 | 2 |
| GS-3 | 2 | 2 | 2 |
| GS-2 | 1 | 1 | 1 |
| GS-1 | 0 | 0 | 0 |
| Subtotal | 432 | 455 | 484 |
| Commissioned Corps (42 U.S.C. 207): | |||
| Assistant Surgeon General | 0 | 0 | 0 |
| Director Grade | 1 | 0 | 0 |
| Senior Grade | 0 | 0 | 0 |
| Full Grade | 1 | 0 | 0 |
| Senior Assistant Grade | 0 | 0 | 0 |
| Assistant Grade | 0 | 0 | 0 |
| Subtotal | 2 | 0 | 0 |
| Ungraded | 224 | 233 | 242 |
| Total permanent positions | 433 | 449 | 499 |
| Total positions, end of year | 659 | 689 | 727 |
| Total full-time equivalent (F T E) employment, end of year | 601 | 632 | 707 |
| Average ES salary | 182,850 | 183,500 | 184,152 |
| Average GM/GS grade | 12.8 | 12.9 | 12.9 |
| Average GM/GS salary | 125,752 | 130,458 | 137,573 |
1 Includes FTEs whose payroll obligations are supported by the NIH Common Fund.